Schizophrenia Symptoms vs Personality Disorder Symptoms How to Tell Them Apart
· 19 min read

If you are reading this, chances are you have noticed something unsettling. Maybe your loved one hears voices that are not there, or maybe they swing between deep distrust and desperate clinginess in a way that feels impossible to understand. You are trying to figure out what is actually going on, and you keep hitting dead ends.

Is this schizophrenia? Could it be a personality disorder like borderline (BPD) or avoidant personality disorder? The truth is that schizophrenia symptoms such as hallucinations, disorganized speech, and social withdrawal can closely resemble the emotional turmoil and distorted thinking seen in certain personality disorders. This overlap is real, and it causes a staggering amount of misdiagnosis.
When a doctor or therapist gets the diagnosis wrong, the treatment plan misses the mark. Someone with schizophrenia might be given therapy meant for BPD symptoms, or vice versa. That delay in proper care does real harm. Patients get sicker, families feel more lost, and trust in the mental health system erodes. According to the World Health Organization, schizophrenia affects approximately 23 million people worldwide, yet many of them are initially mislabeled. The same confusion happens with conditions like avoidant personality disorder, where someone’s extreme fear of rejection can look like the negative symptoms of schizophrenia. And during an existential crisis, brief psychotic episodes can mimic schizophrenia, adding another layer of complexity.
This guide is built to clear up that confusion. We will walk through the key differences step by step using plain language and real research. You do not need a medical degree to follow along. By the end, you will know exactly which signs point to schizophrenia and which point to a personality disorder, and you will know what to do next. If you want a broader map of the main personality disorder groups first, check out our breakdown of the 10 personality disorder types grouped by cluster. It will give you a solid foundation for the comparisons ahead.
Understanding Schizophrenia Symptoms
Now that you have the personality disorder map in mind, let us zoom in on schizophrenia. The key to telling these conditions apart starts with knowing exactly what schizophrenia symptoms look like. And here is the thing: they come in three distinct groups that doctors call positive, negative, and cognitive symptoms.
Positive symptoms are the ones most people picture when they hear the word schizophrenia. These are behaviors or experiences that get added to a person’s normal mental life. Hallucinations top the list. A person might hear voices that no one else hears, see things that are not there, or feel sensations that have no real cause. Delusions are another major positive symptom. These are fixed false beliefs that do not change even when presented with clear evidence. For example, someone might believe they are being followed by government agents or that they have special powers. According to the National Institute of Mental Health, schizophrenia affects roughly 0.25% to 0.64% of U.S. adults, and these positive symptoms are often the first sign that something serious is happening.
Negative symptoms are harder to spot because they involve things that are taken away. The person may lose their ability to feel pleasure or show emotion. Their face might go flat and expressionless no matter what is happening around them. They stop talking much and withdraw from friends and family. This part of schizophrenia is what gets confused with conditions like avoidant personality disorder or severe depression. When you see a loved one becoming distant and quiet, it is easy to assume they are just shy or sad, but the root cause in schizophrenia is very different.

Cognitive symptoms affect how the brain processes information. Someone might struggle to pay attention during a conversation. Their memory may slip, making it hard to keep track of appointments or to learn new things. They might also have trouble making decisions or solving everyday problems. These deficits are not about intelligence. They are about how the brain organizes and uses information. The annual number of new schizophrenia cases worldwide sits at about 1.2 million, as reported in the schizophrenia statistics for 2026 from SingleCare, which shows this is not a rare condition at all.
Here is the bottom line. When you compare schizophrenia symptoms to BPD symptoms or avoidant personality disorder patterns, look for the combination of all three symptom groups. Personality disorders usually do not include full-blown hallucinations or the kind of cognitive decline seen in schizophrenia. If you want to go deeper on how emotional instability compares across these conditions, our guide on emotional dysregulation and how it differs from psychosis and personality disorders lays out the differences clearly.
Positive Symptoms
Let’s dig into the most noticeable signs of schizophrenia. Positive symptoms are called "positive" because they add experiences to a person’s mind. They are not good in any way. They are intense and often scary.
The biggest one is hallucinations.
Most often, people hear voices that are not there. These voices might comment on what they are doing, talk to each other, or give commands. Less often, they might see things or feel things that do not exist. Then there are delusions. These are rock-solid false beliefs. Someone might think they are being watched, that they have secret powers, or that strangers are plotting against them. No amount of proof changes their mind. According to the official DSM-5 criteria for schizophrenia, these are the two main positive symptoms.
But there is more. Disorganized speech and behavior also fall under positive symptoms. A person’s words might jump between topics with no clear link. They might laugh at sad news or get angry for no reason. Their actions can become strange or pointless, like dressing in heavy coats on a hot day.
Here is the key. If you see hallucinations or strong delusions in someone, that points toward schizophrenia, not toward most personality disorders. Personality disorders like BPD or avoidant personality disorder do not cause full-blown hallucinations. To learn more about all the different personality disorder types and how they compare, check out our guide on the 10 personality disorder types grouped by cluster A, B, and C.
Negative and Cognitive Symptoms
The positive symptoms we covered get a lot of attention. But the negative and cognitive symptoms are the ones that often cause the most long-term trouble. They are quieter, though they deeply affect daily life.
Negative symptoms mean a loss of normal abilities. A person might have avolition, which is a lack of drive. They stop doing basic things like showering, cooking, or going to work. Another is alogia, meaning they speak very little. When asked a question, they might give one-word answers or stay silent. They also pull away from people. This social withdrawal is not about being shy. It feels like a wall has gone up between them and the world. These symptoms are often chronic and stick around even when treatment is helping. The official DSM-5 definition and chronic nature of schizophrenia confirms how these deficits are a core part of the disorder.
Cognitive symptoms affect how a person thinks. Memory gets shaky. They might forget what you just said or lose track of important dates. Attention fades easily. Watching a full movie or reading a page in a book can feel impossible. Planning and organizing also become very hard. Simple tasks like paying bills or following a recipe feel overwhelming.
It can be confusing to watch a loved one go through this. You might wonder if they are just lazy or unmotivated. But these are real brain-based symptoms. To better tell the difference between a lack of drive and other mental health issues, read our guide on emotional dysregulation and how it differs from psychosis.
Recognizing Personality Disorder Symptoms
Now, here is where things can get tricky. Some personality disorders look a lot like schizophrenia symptoms at first glance. This is especially true for Cluster A disorders.
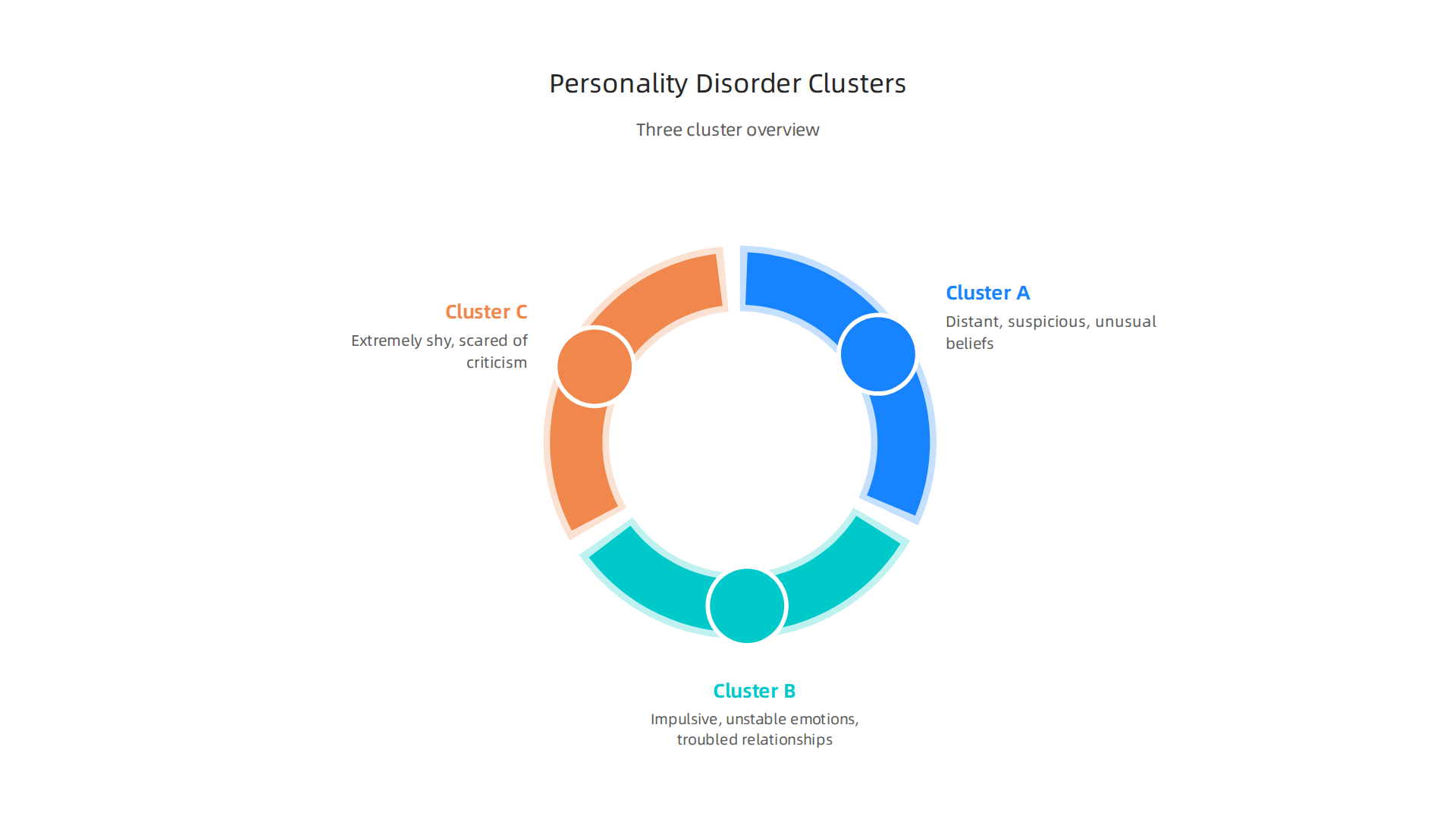
Personality disorders are broken into three groups. Cluster A covers the odd or eccentric types. This includes paranoid personality disorder, schizoid personality disorder, and schizotypal personality disorder. People with these conditions may seem distant, suspicious, or disconnected from social norms. The DSM-5 definition of Cluster A personality disorders describes behaviors that can resemble the negative symptoms of schizophrenia. But there is a key difference. People with Cluster A disorders do not have active psychosis that comes and goes. They do not have clear hallucinations or delusions that define schizophrenia.
Cluster B includes dramatic and emotional disorders. Examples are borderline personality disorder, antisocial personality disorder, and narcissistic personality disorder. If you have seen bpd symptoms before, you know they involve mood swings, fear of abandonment, and unstable relationships. These differ from schizophrenia because the person stays in touch with reality, even when emotions run high.
Cluster C covers anxious and fearful types. These are avoidant personality disorder, dependent personality disorder, and obsessive-compulsive personality disorder. Someone with avoidant personality disorder feels extremely shy and scared of rejection. That is not the same as the social withdrawal in schizophrenia.
The real test is time. Personality disorders start early in life and stay stable. Psychotic conditions like schizophrenia tend to show up later and can change over time. For a clearer breakdown of all ten types and how they compare, check out our guide to the 10 personality disorder types grouped by cluster.
This can feel confusing when you are trying to help a loved one. But knowing the difference matters for getting the right support.
Cluster A, B, and C Overview
To help you tell these apart more clearly, here is a simple look at each personality disorder cluster.
Remember, knowing these differences is key when comparing them to schizophrenia symptoms.
Cluster A: Odd or Eccentric
This group includes paranoid, schizoid, and schizotypal personality disorders. People with these conditions may seem distant, suspicious, or have unusual beliefs. But they do not lose touch with reality the way someone with schizophrenia does. For a deeper look at one type, check out our guide on schizoid personality disorder symptoms.
Cluster B: Dramatic or Emotional
This cluster includes borderline, histrionic, narcissistic, and antisocial personality disorders. The main features are impulsiveness, unstable emotions, and trouble keeping relationships. BPD symptoms can sometimes be confused with mood disorders, but the pattern is long-standing. The Cleveland Clinic overview of Cluster B personality disorders explains the traits in more detail.
Cluster C: Anxious or Fearful
This group covers avoidant, dependent, and obsessive-compulsive personality disorders. People with avoidant personality disorder are extremely shy and scared of criticism. Dependent personality disorder involves a strong need to be taken care of. Obsessive-compulsive personality disorder is about perfectionism, not the same as OCD.
The Merck Manuals overview of personality disorders groups all ten types by cluster. Using this framework helps you see which behaviors match a personality disorder and which might point to something like schizophrenia.
Overlap with Schizophrenia
Now let’s look at where some personality disorders and schizophrenia symptoms actually cross paths. This happens most often with two types.
Schizotypal personality disorder shares odd beliefs, strange speech, and unusual perceptions with schizophrenia. But in schizotypal, these are milder and don’t include full-blown psychosis. For more detail, read this schizotypal personality disorder overview. The big difference? People with schizophrenia lose touch with reality for longer periods.
Borderline personality disorder (BPD) can include brief psychotic episodes under high stress. Someone might hear voices or become paranoid for a few hours or days. This overlaps with schizophrenia, but the key is timing. The confusion between BPD and schizophrenia overlap happens because both can involve psychosis. However, BPD symptoms tend to come and go with stress, while schizophrenia symptoms are more constant and independent of life events.
Duration and context are everything. A Kaiser Permanente study on co-occurring schizophrenia and BPD found that when both conditions exist together, outcomes get worse. That is why getting the right diagnosis matters so much. You can learn more in our guide comparing schizophrenia symptoms vs personality disorder symptoms.
Key Differences Between Schizophrenia and Personality Disorders
Now that you see how some personality disorders overlap with schizophrenia, let’s look at what makes them different. Knowing these differences can help you understand why doctors separate them. Here are three big ones.
Age of onset. Schizophrenia usually shows up in late adolescence or early adulthood. A person might first experience hallucinations or delusions around age 18 to 25. A schizophrenia overview from the NIH notes that siblings often develop the disorder at the same age, which points to a strong genetic link. Personality disorders are different. They often start earlier in life and keep going. Traits like odd behavior or social withdrawal can appear in childhood or early teens. The Cleveland Clinic overview of personality disorders explains that these patterns are long-lasting and start by early adulthood at the latest.
Symptom stability. Here is another major difference. Schizophrenia symptoms tend to come in episodes. A person might have a psychotic break, get treatment, feel better for months, and then have another relapse. The symptoms can go away and come back. Personality disorders do not work that way. They are pervasive and stable over time. If someone has a personality disorder, those traits are always there. They do not disappear between episodes. An article from University Behavioral Health titled Is Schizophrenia a Personality Disorder? describes how the two conditions are distinct because personality disorders are a fixed part of who someone is, while schizophrenia can flare up and calm down.
Treatment response. This difference matters a lot for getting better. Schizophrenia almost always needs antipsychotic medication. The Mayo Clinic schizophrenia diagnosis and treatment page confirms that lifelong treatment with medicine and therapy helps manage symptoms. Without medication, the psychotic symptoms usually return. Personality disorders respond best to psychotherapy. Medicine may help with related issues like anxiety or depression, but it does not fix the core personality pattern. For example, a Schizoid Personality Disorder vs Schizophrenia guide shows that schizoid personality disorder rarely requires medication and focuses on therapy instead. Want to learn more about the different types? Check out our guide to the 10 personality disorder types grouped by cluster to see where each one fits.
Getting the right diagnosis changes everything. If doctors mix up schizophrenia with a personality disorder, the treatment plan will be wrong. That can waste time and make things worse. Understanding these three differences age of onset, symptom stability, and treatment response helps you see why experts keep them separate.
Diagnostic Challenges and Comorbidity
Even for trained professionals, telling these conditions apart can be tricky. Here is why.
One big problem is that schizophrenia and personality disorders often happen together. Studies show that up to 40% of people with schizophrenia also meet the criteria for a personality disorder. This is called comorbidity. For example, bpd symptoms like unstable emotions and impulsive actions can show up alongside schizophrenia symptoms like hallucinations. The combination makes it hard to know which condition is driving the problem. A review of the research on the co-occurrence of psychotic disorders and borderline personality disorder says this overlap complicates clinical management and makes symptoms worse.
Another challenge is misdiagnosis. A doctor might see a patient who is withdrawn and talking oddly. Based on that one moment, they might think it is schizophrenia. But if they looked at the person’s whole life story, they might find a long pattern of odd beliefs and social isolation that started in childhood. That pattern points more toward a personality disorder like schizotypal personality disorder. The Schizotypal Personality Disorder overview from StatPearls explains that this condition involves lifelong deficits in forming close relationships, not sudden psychotic breaks. When clinicians only focus on what is happening right now (cross-sectional symptoms) instead of the person’s history over time, mistakes happen.
So how do experts get it right?
They use two main tools. First, structured clinical interviews. These are standard sets of questions that dig into a person’s past and present symptoms in a consistent way. Second, they collect collateral information. That means talking to family members or looking at old medical records. This gives a fuller picture of how long symptoms have been present and how stable they are. If you want to understand more about how emotional ups and downs differ from psychosis, our article on emotional dysregulation and how it differs from psychosis and personality disorders breaks it down clearly.
Getting the diagnosis right matters because treatment changes so much depending on the condition. When comorbidity is present, the treatment plan has to address both the psychotic symptoms and the personality pattern. That takes a careful, informed approach.
Case Examples: When Symptoms Overlap
Now let’s look at two real-world examples that show how these overlaps play out in practice.
Case 1: Transient Psychotic Symptoms in BPD Mistaken for Schizophrenia
A 29-year-old woman comes to a clinic saying she hears voices telling her she is worthless. She also reports feeling empty and has a history of cutting her arms when upset. The voices only appear during times of extreme stress, like after a breakup. Within a few days, they go away on their own. Her mood swings are fast and tied to relationship problems, not gradual. The pattern fits bpd symptoms more than schizophrenia symptoms. A study on the contrasting characteristics of psychosis in BPD versus schizophrenia found that psychotic symptoms in BPD are often short-lived and triggered by stress, while in schizophrenia they tend to be more constant and unrelated to events. Without a careful history, a doctor might wrongly diagnose schizophrenia and start antipsychotics that are not really needed.
Case 2: Odd Beliefs or Schizophrenia Prodrome?
A 22-year-old man believes he has special powers to read people’s thoughts. He lives alone, has no close friends, and dresses in unusual ways. He has never had a clear hallucination or a full delusion that makes him act dangerously. His mother says he has been "different" since elementary school, always keeping to himself and talking about strange ideas. This lifelong pattern points toward schizotypal personality disorder, not the beginning of schizophrenia. A list of conditions that can seem like schizophrenia explains that people with schizotypal personality disorder have odd beliefs and social isolation but do not experience the same level of psychotic breaks. The key difference is that their oddness is stable over years, not a new problem that gets worse.
These cases show why doctors must look at the full story. They need to ask how long symptoms have lasted, what triggers them, and whether there is a family history of psychosis. For a deeper dive into how to tell these conditions apart, check out our guide on schizophrenia symptoms vs personality disorder symptoms. Getting it right changes the whole treatment path.
Next Steps: Seeking Help and Support
By now you have a clearer picture of how schizophrenia symptoms can look like personality disorder symptoms and vice versa. That knowledge is powerful, but knowing is only half the battle. The real next step is getting the right kind of help.
Start With a Comprehensive Evaluation
If you or someone you care about is experiencing any of the symptoms we have discussed, do not try to figure this out alone. The smartest move is to see a psychiatrist for a full evaluation.

A good psychiatrist will take a detailed history, talk to family members if possible, and rule out other conditions before landing on a diagnosis. They will ask about how long symptoms have lasted, what triggers them, and whether there is a family history of mental illness. This process can take more than one visit, and that is normal. A quick label is not helpful. A careful one changes everything.
The American Psychiatric Association recently released updated recommendations for treating schizophrenia, and they stress that a proper diagnosis comes first. You can read more in the APA practice guideline on schizophrenia treatment to understand what a thorough evaluation should include.
Treatment Options Depend on the Diagnosis
Once a clear diagnosis is made, treatment follows a specific path.
For schizophrenia, the standard approach combines medication with psychosocial support. Antipsychotic medicines help reduce or stop hallucinations and delusions. Therapy, job training, and family support help people rebuild their lives. The most effective care uses both together. The latest research shows that comprehensive treatment for schizophrenia works best when medication and therapy happen at the same time, not one without the other.
For personality disorders, the treatment is different. Medications are not the main answer. Instead, therapies like dialectical behavior therapy (DBT) and cognitive behavioral therapy (CBT) help people understand their emotions, change unhelpful patterns, and build healthier relationships. These therapies take time and practice, but they can make a real difference.
If you are still unsure which direction fits your situation, take a look at our guide on the 10 personality disorder types grouped by cluster. It breaks down each condition in plain language so you can see where your symptoms might fit.
One Final Thought
Getting the right help starts with asking the right question. Depression education needs context, not confusion. If you feel stuck, visit Ask a Better Question to find more resources that can point you toward clarity and the right kind of support.
You do not have to figure this out alone.

A good professional, the right information, and a little patience can make all the difference.
Summary
This article explains why schizophrenia symptoms often look like certain personality disorders and how that overlap leads to frequent misdiagnosis. It describes schizophrenia’s three symptom groups—positive (hallucinations, delusions, disorganized speech), negative (withdrawal, flat affect), and cognitive (memory and attention problems)—and contrasts them with Cluster A, B, and C personality disorder patterns. The guide highlights key differences in age of onset, symptom stability, and treatment response so you can judge whether psychosis or a long‑standing personality pattern fits better. It shows common trouble spots, such as brief stress‑related psychosis in borderline personality disorder and lifelong oddness in schizotypal cases, and explains why clinicians use structured interviews and family history to decide. Practical next steps cover when to seek a psychiatrist, what to expect in an evaluation, and how treatment plans differ. By reading this, you’ll be better able to spot red flags, ask informed questions, and push for the right diagnosis and care for yourself or a loved one.